Document Type : Case Reports
Authors
Dept. of Oral Medicine, shahid Beheshti University of Medical Sciences, Tehran, Iran
Abstract
Giant Cell Fibroma (GCF) was described as a new entity of fibrous hyperplastic soft tissue. It seems that stimulus from an unexplained origin can have a role in its etiology. Histopathologically GCF is consisted of multinucleated fibroblasts that have oval shape nuclei within the eosinophilic cytoplasm. Surgical excision is the treatment of choice and recurrence is very rare. Here we report a case of relatively large GCF in a 54-year-old man. Gingiva is the common location of GCF. As in our case, it may be mistaken as irritation fibroma especially if it is on the buccal mucosa, the most common location for fibroma. Correct diagnosis is based on biopsy and clinical examination to see surface texture roughness. To minimize bleeding because of its large size an excisional biopsy with Diod laser was performed under local anesthesia for this patient.
Keywords
Main Subjects
Introduction
Giant Cell Fibroma (GCF) was first described by Weathers and Calliham as a new entity of fibrous hyperplastic soft tissue in 1974. GCF is a relatively rare fibrous lesion and very few case reports are available regarding this lesion (1). It represents 2-5% of all biopsied fibrous lesions of oral cavity (2). There is controversy about the origin of GCF (1). It seems that stimulus from an unexplained origin can have a role in its etiology (2). GCF occurs commonly in patients under the age of 30 years with a slight female predilection.
Gingiva followed by the tongue and buccal mucosas are most involved locations (3). It appears as a pedunculated or sessile asymptomatic exophytic lesion with size of less than one cm in the oral cavity. Like irritation fibroma it is a reactive fibrous proliferation with some discriminative differences such as surface texture, which is not smooth. Histopathologically GCF consists of multinucleated fibroblasts in close relation with overlaying epithelium within avascular collagenic stroma. These fibroblasts have oval shape nuclei within the eosinophilic cytoplasm esembling a stellate appearance (1,4-6). Positive reactivity for vimentin (but not for cytokeratin, neurofilament, HHF, CD 68, HLA DR, tryptase and S100) suggests a fibroblastic phenotype. Surgical excision is the treatment of choice and its recurrence is very rare (2)
Although GCF presents more frequently in young adults and in gingiva, it should be considered as a diagnosis in other locations and higher ages. Here we report a case of GCF in an elderly male.
Case Presentation
A 54-year-old man presented to Oral Medicine Department with chief complaint of an oral lesion since 3 years ago. He was edentulous and was referred by her dentist for further evaluation prior to making prosthesis. His social and medical history was not remarkable but his habitual history revealed smoking 1 pocket of cigarette per day for 35 years.
An informed consent was taken from the patient and all ethical issues were observed.
Intra oral examination revealed an exophytic sessile lesion on the right buccal mucosa (Fig. 1) with no pain or tenderness. The lesion was round in shape and its color was like the normal surrounding mucosa with hyperkeratosis on its surface due to trauma. Surface texture was granular and the lesion was firm on palpation. The size of the lesion was 15×12 mm.
With respect to the clinical manifestation and its location as well as high possibility of trauma to the buccal mucosa a provisional diagnosis of irritation fibroma was given and then a differential diagnosis of GCF was also considered due to the surface texture. For definitive diagnosis and as a treatment excisional biopsy was considered. To minimize bleeding because of its large size an excisional biopsy with Diode laser (Dr. Smile, Italy) was performed under local anesthesia and no suture was required to stop bleeding. The patient was advised not to smoke during healing period to prevent delayed wound healing. Histopathology examination showed a nodular mass of fibrous connective tissue composed of numerous large stellate fibroblasts and collagen bundles arranged in radiating and circulating fashion. The lesion was covered by nonkeratinized to orthokeratinized-stratified squamous epithelium with elongated rete ridge and papillary at surface (Fig. 2, 3).

Fig. 1: Intra oral examination shows a pedunculated mass in the right buccal mucosa of the mouth. In this view the pedunculated growth with pebbly appearance of the surface is seen

Fig. 2: Intra oral view 2 weeks after laser excision
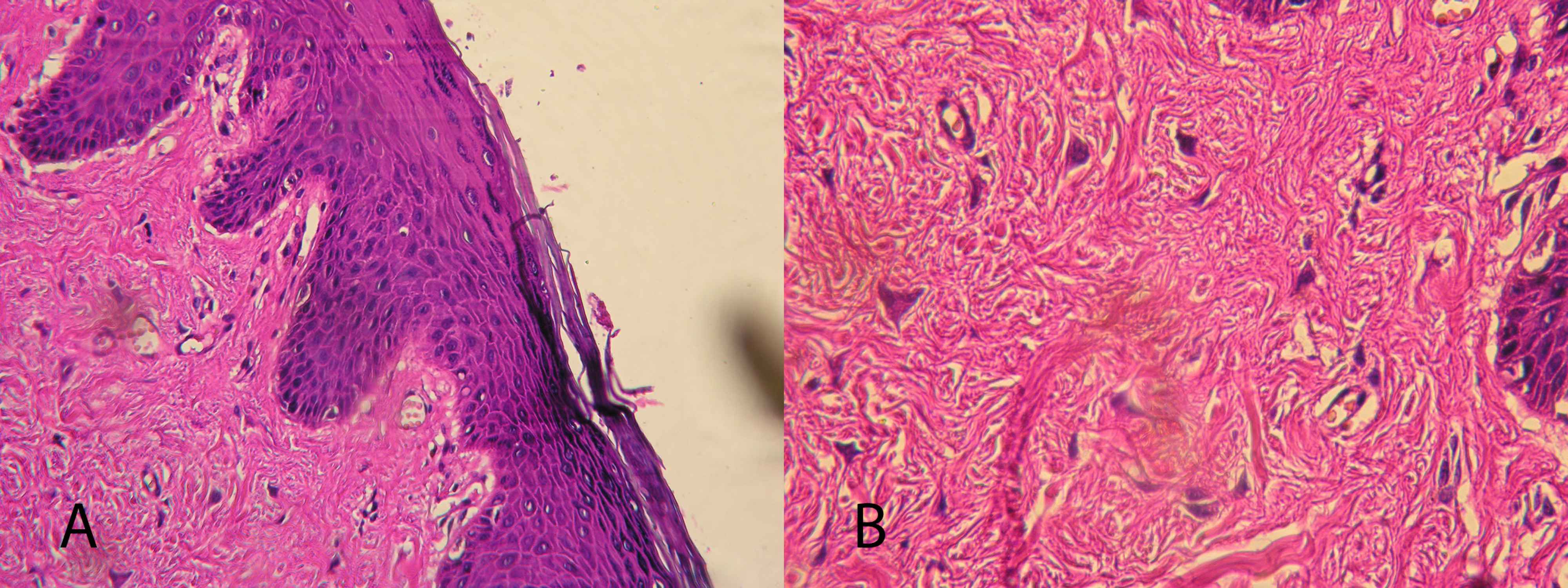
Fig. 3: A) Hematoxilin and eosin stained tissue sections of the lesion showing stratified squamous epithelium with elongated rete ridges as well as numerous characteristic large plump stellate fibroblasts mostly located in the surface connective tissue especially near epithelium.(Magnification 200). B) Hematoxilin and eosin stained tissue sections of the lesion showing numerous large stellate fibroblasts and dense collagen fibers within the fibrovascular connective tissue. (Magnification 400)
Discussion
GCF is a relatively rare lesion clinically similar to hyperplasia with some particularities, which differentiate it from other entities (7). Usually it presents as a pedunculated or sessile, asymptomatic growth with nodular surface and 0.5 to 1 cm diameter (8). Our case had similar findings. It may occur at any age but 29 and 39 years of age are mentioned in the literature as it means age development (1). Magnusson and Rasmussen reviewed 103 cases of GCF and reported that the mean age was 27.7 years (9). It is found predominantly in first three decades of life with slight female predilection (8). As an elderly male, our patient was out side the common age group for GCF. Our patient is an elderly male while the majority of large studies found a female preponderance for occurrence of GCF (5, 10). However, Sabarinath et al. (1) showed a slight male predominance in a survey consisting of 21 cases and few studies have reported equal sex predilection (8). Caucasians are the most racial group involved (3) and our patient was a Caucasian too. Sabarinath et al. reviewed 21 oral GCF and concluded that it is an asymptomatic lesion with the color of normal mucosa and granular surface (1). These characteristics were the same in our case.
The most frequently site in the oral cavity is gingiva followed by the tongue and buccal mucosa (1) and mostly of them are less than 1 cm in diameter with the average size under 0.5 cm (4). In our case the lesion was in the buccal mucosa, the location that is not very common and was markedly bigger than usual size, which is determined in the literatures.
The clinical presentation of the majority of no neoplastic growths in the oral cavity is similar and differentiation depends on histopathology features. According to clinical features, fibroma fibroepithelial polyp, pyogenic granuloma and fibrous hyperplasia are differential diagnosis although GCF has definitive histological features (7, 8).
In relation to histopathology, GCF is a mass showing fibrous connective tissue with the presence of large spindle shaped or more often stellate shaped cells being the most characteristic feature (5). These large cells have marked cell borders and those located near the epithelium may have granules with melanin characteristics (8). Overlaying epithelium is keratinized stratified squamous with elongated rete ridges (1).
Positive reactivity for vimentin as well as negativity for S-100, alpha smooth muscle actin, CD8 leukocytes common antigen (LCA) and HLA-DR confirm fibroblastic origin and rule out melanocyte, Langerhans, endothelial, myofibroblast and macrophage-monocyte lineage (8, 2).
Pathologic examination revealed the same features in our case. So some clinical features of the lesion in our case, the same as asymptomaticity and pink color was in agreement with the clinical features described by Weathers and Callihan (11), but from the view point of location, size, age and sex involvement was not correlated with literatures. It was larger than normal size, not in usual location and in an elderly man, which is not in common age group.
Conclusion
Although GCF is a rare entity that mostly occure in younger adults but it may be considered in differential diagnosis of exophytic lesions of the oral cavity even in elderly patients.
Acknowledgements
We appreciate close cooperation of the Oral Medicine Department of Dental School, Shahid Beheshti University of Medical Sciences. The authors declare that there is no conflict of interests.
- Sabarinath B, Sivaramakrishnan M, Sivapathasundharam B. Giant cell fibroma: A clinicopathological study. J Oral Maxillofac Pathol 2012;16:359-62.
- Jimson S, Jimson S. Giant cell fibroma: a case report with immunohistochemical markers. J Clin Diagn Res 2013;7:3079-80.
- Kuo RC, Wang YP, Chen HM, Sun A, Liu BY, Kuo YS. Clinicopathological study of oral giant cell fibromas. J Formos Med Assoc 2009;108:725-9
- Bakos LH. The giant cell fibroma: a review of 116 cases. Ann Dent. 1992;51:32-5.
- Houston GD: The giant cell fibroma: a review of 464 cases. Oral Surg Oral Med Oral Pathol 1982;53:582-7.
- Weathers DR, Campbell WG. Ultrastructure of the giant cell fibroma of the oral mucosa. Oral Surg Oral Med Oral Pathol 1974;38:550-61.
- Braga MM, Carvalho AL, Vasconcelos MC, Braz-Silva PH, Pinheiro SL. Gianty cell fibroma:a case report. J Clin Pediatr Dent 2006;30(3):261-4.
- Sonalika WG, Sahu A, Deogade SC, Gupta P, Naitam D, Chansoria H, et al. Giant cell fibroma of tongue:Understanding the nature of an unusual histopathological entity. Case Rep Dent 2014;2014:864512.
- Magnusson BC, Rasmussen LG.The giant cell fibroma. A review of 103 cases with immunohistochemical findings. Acta Odontol Scand 1995;53:293-6.
- Wang Z, Levy B. Clinico-pathological study on giant cell fibroma of oral mucosa. Zhonghua Kou Qiang Yi Xue Za Zhi 1995; 30:332-3, 383.
- Weathers DR, Callihan MD. Giant cell fibroma. Oral Surg Oral Med Oral Pathol 1974;37: 374-384.
)